Let the Random Variable X Represent the Number of Boys in a Family With Three Children
![]()
Schoolhouse Readiness in 4-Year-Former Very Preterm Children
by ane,2,*  , 1 , one,2 , ane , 1 , 1,2 , 3 and 4
, 1 , one,2 , ane , 1 , 1,2 , 3 and 4
1
Abigail Wexner Research Institute, Nationwide Children'south Hospital, Columbus, OH 43215, USA
2
Section of Pediatrics, The Ohio Land Academy, Columbus, OH 43210, U.s.
3
Section of Epidemiology, Rollins Schoolhouse of Public Health, Emory University, Atlanta, GA 30322, United states
four
Department of Pediatrics, Emory University, Atlanta, GA 30322, USA
*
Author to whom correspondence should be addressed.
Academic Editors: Lianne Woodward and Mandy Brown Belfort
Received: ten January 2022 / Revised: ten Feb 2022 / Accepted: 21 February 2022 / Published: 1 March 2022
Abstract
The aims of this study were to identify the aspects of school readiness that all-time distinguish very preterm (VPT) preschoolers from full-term (FT) controls, determine the extent to which readiness problems in the VPT group reflected global cognitive weaknesses or more than specific deficits, and identify singled-out profiles of readiness problems. 50-three VPT (gestational age ≤ 30 weeks) 4-twelvemonth-olds were compared to 38 FT (gestational age ≥ 37 weeks) controls on measures of global cerebral ability, executive function, motor skills, early literacy and numeracy, and psychosocial functioning. Latent course analysis (LCA) was also conducted to identify individual readiness profiles. The VPT grouping had the near pronounced difficulties on tests of spatial and nonverbal cerebral abilities, executive role, motor skills, phonological processing, and numeracy. The VPT group as well had sex activity-related difficulties in processing speed, social operation, and emotion regulation. These differences were evident in analyses of both continuous scores and rates of deficits. The VPT grouping's difficulties in motor skills, and VPT females' difficulties in social performance and emotion regulation, were axiomatic even when controlling for global cognitive power. LCA suggested four profiles of readiness, with the majority of the VPT group assigned to profiles characterized by relative weaknesses in either cognitive abilities or psychosocial operation or by more than global readiness problems. The findings support the need to evaluate multiple aspects of schoolhouse readiness in VPT preschoolers and inform efforts to pattern more targeted early educational interventions.
1. Introduction
Very preterm (VPT) children, typically defined every bit those born at a gestational age (GA) < 32 weeks, are at higher take chances for deficits in academic achievement than full-term (FT) children [1,2]. These issues persist across the school-age years, are inversely related to the caste of prematurity at birth, and are preceded by before developmental delays [1,2,3,4,5,6].
According to the American Academy of Pediatrics [7] and an updated technical report [viii], school readiness covers a broad range of characteristics conducive to learning, including health and physical/motor development, social–emotional adjustment, approaches to learning as exemplified by motivation and self-command, advice skills, and general knowledge (including knowledge of letters and numbers) and cognition. More recently, the concept of school readiness has been expanded to include factors outside the child, such as family, school, and community supports, that can foster readiness if nowadays or hamper information technology if absent [8,9]. In an Australian sample, a delay in at least one of these characteristics was observed for 44% of VPT v-year-olds compared to 16% of FT controls [10]. Researchers in New Zealand documented generalized delays in schoolhouse readiness skills at age 4 years in VPT children compared to FT controls [four]. In the latter study, delays in multiple areas of readiness were three times more common in the VPT group compared to the FT group and predicted after deficits in bookish achievement at ages half dozen and ix years. Other studies provide additional evidence for deficits in cognitive and emotional cocky-regulation in VPT preschoolers and associations of these deficits with learning problems [11,12,13,14,15,16,17,18,xix].
Findings indicating that some VPT children accept selective deficits in executive role, motor skills, and mathematics, while others appear free of any discernable impairments, raises the possibility of private variability in school readiness profiles [xx,21,22]. Individual variability is also supported by findings that suggest unlike profiles of school readiness skills in community samples of children [9,23,24] and of behavior bug in extremely preterm (GA < 28 weeks) children [25]. Using cluster or latent class analysis (LCA), these studies identified profiles suggesting that some children take pervasive bug in readiness skills or beliefs while others have more selective deficits or are functioning well in all areas.
Findings from two more recent studies that employed LCA provide additional support for different profiles of cognitive, motor, and behavior outcomes at early school age. In following a large French sample of VPT children (GA < 32 weeks) to age 5.5 years for the EPIPAGE-ii Study, Twilhaar and colleagues [26] identified four profiles of cognitive, motor, and psychosocial characteristics. One profile was characterized by outcomes that were comparable to those of a FT sample, a second by more than difficulties in psychosocial adjustment than in cognitive and motor skills, a third by more problems in cognitive and motor abilities than in psychosocial adjustment, and a quaternary by difficulties in all areas relative to the FT children. A report of some other sample of 5-year-old VPT children (GA < 30 weeks) and a FT comparing group too identified four profiles [27]. 1 profile was characterized by age-typical cognitive, motor, language, and psychosocial characteristics, a second by balmy cognitive, motor, and language deficits in the context of more typical psychiatric ratings, a third past parent reports of pronounced psychosocial problems, and a fourth by instructor reports of relatively severe symptoms of attention issues and autism spectrum disorder.
However, evidence of individual differences in profiles of school readiness among VPT preschoolers is limited. The relationship betwixt cognitive or motor deficits and behavior problems in these children is also unclear. Although cognitive impairments are associated with behavior problems in VPT cohorts [28,29,30], further enquiry is needed to examine the possibility of relatively isolated deficits in behavior or performance-based measures of cognitive and motor functioning in preschoolers.
The objectives of this written report were to enhance knowledge of the effects of VPT nativity on school readiness in 3 ways. First, we compared groups of VPT preschoolers and FT controls on multiple measures of readiness to identify the breadth and magnitude of readiness issues in the VPT group and to confirm that our cohort had deficits similar to those observed in seminal studies of VPT preschoolers [8,9,10,13,17,20,24,25,26]. The two groups were compared on both continuous measures of readiness and rates of deficits on these measures. A second objective was to examine the extent to which problems in different readiness domains varied independently of one some other. Thirdly, we conducted LCA to examine evidence for distinct profiles of readiness and their association with grouping membership.
Data regarding the blazon and magnitude of VPT preschoolers' deficits in readiness will help in targeting interventions for these children's most pressing needs. Testify for distinct types or profiles of deficits will also contribute to an improved understanding of individual variability in readiness issues and will guide in creating assessments of readiness that are sensitive to the total range of readiness problems. Based on research on the consequences of VPT birth in young children, we hypothesized that VPT preschoolers would differ from FT controls on a broad array of readiness measures, only that the magnitude of these differences would vary across measures. Consistent with by testify for individual variability in outcomes of VPT birth, we also anticipated multiple types and patterns of grouping differences.
2. Materials and Methods
2.one. Sample
As described in studies of resilience and positive adaptation in VPT preschoolers [31,32], VPT children were recruited by contacting families of children treated in the Follow-Upwardly programme for a network of neonatal intensive care units affiliated with Nationwide Children'south Hospital in Columbus, Ohio USA. To examine outcomes in a higher-risk VPT preschool sample, only children with GA ≤ xxx weeks were included. Children had to be four years of age at the fourth dimension of recruitment. Children from non-English speaking families and those with genetic abnormalities known to affect cognition were excluded. Given our interests in examining performance-based measures of readiness, we also excluded children with severe sensory impairment. To capture as many children as possible within the recruitment period (September 2018 to June 2019), VPT preschoolers were recruited according to age (older to younger) from a larger hospital-based sample of VPT children. The VPT group comprised 53 of threescore eligible children. Seven children were not seen because of missed or canceled appointments. Comparison of these vii children to the participants failed to reveal significant differences in GA, age at cess, or sex (ps > 0.05). FT controls included 38 children recruited at iv years of historic period during the aforementioned period as the VPT group. Recruitment was from flyers emailed to hospital employees who had volunteered for inquiry.
Tabular array 1 summarizes the nascence and demographic characteristics of the ii groups. The VPT group had a significantly lower z-score composite of SES (zSES) than the FT group (p < 0.001), with zSES defined equally the mean of sample z-scores for measures of caregiver education, occupation, and census-based median family income [33]. The groups did not differ significantly in age at assessment, sex, or race.
2.2. Procedures and Measures
One grouping of examiners administered a battery of readiness tests to the children while dissimilar examiners supervised caregivers' completion of child behavior rating scales. Children's nativity condition was not shared with the child examiners. Child testing was completed in four half-60 minutes sessions spanning approximately iii hours, with breaks between the sessions. Tasks were administered in ane of three orders, with children assigned randomly to an order. The study was canonical by the hospital Institutional Review Lath and caregivers provided informed consent before participation.
Measures of readiness were divided into the five domains listed in Tabular array ii: global cognitive ability, executive function and processing speed, motor skills, early on literacy and numeracy skills, and behavior problems. Because of the extensive measures of behavior bug provided by the Conners Early Babyhood-Parent questionnaire (Conners EC-P) [36], only scores for total behavior issues and for subdomains previously shown to be adversely afflicted by preterm birth were considered [37]. Scores were historic period-adjusted for measures with normative standards. Adjustments were fabricated for chronological rather than corrected age given that schoolhouse readiness is typically evaluated based on historic period since birth. Historic period norms were not bachelor for the Zoo Get No Go Exam [38] and Emotion Regulation Checklist (ERC) [39]; thus, raw scores were used in analyses of these measures. Table two includes brief descriptions of the traits assessed by each measure and citations that document acceptable levels of reliability and validity. Test validity is further documented past previous research with young VPT or very depression birth weight (<1500 g) children using these or similar tests [11,12,40,41,42,43].
2.3. Analysis
Mixed model analyses were used to examine grouping differences. Covariates in these and other analyses included sex and zSES. A random consequence accounted for dependence between sibling participants. The relative magnitudes of group differences were assessed in terms of outcome size (ES).
The possibility that the VPT and FT groups differed forth multiple dimensions of school readiness was examined in ii ways. Start, the in a higher place-noted mixed model analyses were repeated decision-making for the Differential Ability Scales, 2nd Edition General Conceptual Ability (DAS-Two GCA) [44] to determine if grouping differences could be attributed to differences in global cognitive ability. 2d, a general estimating equation (GEE) analysis was conducted to examine the possibility of multiple independent associations of readiness measures with grouping membership. Predictors in this assay were limited to the one measure out from each of the 5 domains that discriminated the groups with the largest ES.
Additional analyses using GEE were conducted to compare the groups (coded as FT = 0 and VPT = i) on rates of deficits. Deficits were defined as scores ≥ 1SD beneath the hateful on the operation measures and ERC Emotion Regulation, and scores ≥ 1SD above the mean on all ratings of behavior problems except for ERC Emotion Regulation. To determine if the groups differed in rates of deficits, the number of deficits was tallied across individuals, and the groups were compared on rates of ii or more deficits. Although grouping differences in analyses using both mixed models and GEE were like whether scores were adjusted for chronological age or for GA, just results from assay of scores adjusted for chronological age are reported hither.
Because of the descriptive nature of the written report and limited sample size, an uncorrected p-level of <0.05 was applied to make up one's mind statistical significance. Information on the magnitude of effects (EFs) was provided by Cohen's d for group comparisons on continuous measures and by odds ratios (and 95% conviction intervals) for results from GEEs. Small, medium and large effects from mixed models were defined as Cohen's d's of 0.2, 0.5, and 0.viii, respectively [51]. Cohen's d was calculated using the estimated marginal means and standard errors. These values adjust for the effects of the covariates (e.g., zSES) on the point estimates.
LCA was used to investigate individual differences in profiles of deficits. Variables included in these analyses were nearly of those listed in Table 2. Measures excluded from these analyses were the DAS-II GCA in order to focus on potential variations across profiles in the verbal, nonverbal, and spatial ability scores. Subscales of the Behavior Rating Inventory of Executive Part-Preschool (BRIEF-P) [50] and Movement Cess Bombardment for Children, 2nd Edition (MABC-2) [47] were likewise excluded to limit the number of variables. The Children'south Examination of Phonological Processing, 2nd Edition (CTOPP-ii) [46] rapid naming tests were excluded because of missing data due to many children's inability to consistently name the stimuli. Analyses were conducted using Mplus version eight and SAS nine.four. For families with multiple participants, ane child from each family unit was randomly selected to avert biases related to family clustering, with preference given to children with the most consummate data. Seventeen children (15 PT, two FT) were excluded on this basis, resulting in a total sample of 75 children for LCA (39 VPT, 36 FT).
LCA models were run with 1 to 5 latent classes. To determine the best-fitting model, each model was compared to the model with 1 fewer form. The best-plumbing fixtures model was selected based on fit statistics and interpretability. Model fit was assessed using the Bayesian information criteria (BIC), Akaike data criteria (AIC), adapted BIC, Vuong–Lo–Mendell-Rubin test, Lo–Mendell examination, and bootstrap likelihood ratio exam. Lower values on BIC, AIC and adjusted BIC indicated better model fit. A significant p-value on the Vuong–Lo–Mendell–Rubin test, Lo–Mendel-Rubin test, or bootstrap likelihood ratio test indicated a better fit for the less parsimonious model (east.g., the 2-class over the ane-class model). In one case the best-plumbing equipment model was determined, information technology was used to allocate children into their most likely class. Entropy was used to determine nomenclature accuracy. The value of entropy ranges from 0 to one, with higher values indicating better accuracy. Finally, analyses of variance were conducted to compare the children assigned to each course on the readiness measures, group membership, sex, and zSES.
three. Results
3.i. Group Differences in Continuous Measures of Readiness
The VPT group had significantly lower scores on all tests except the NIH Toolbox Dimensional Change Card Sorting Examination [45] and all caregiver behavior ratings except the Conners EC-P Global Index, Inattention/Hyperactivity, and Anxiety scales, Brief-P Inhibitory Self-Command indices, and Flexibility indices, and ERC Lability/Negativity (encounter Table 3). Large ESs were found for DAS-Two GCA, Nonverbal Ability, Spatial Ability, Think of Digits-Forward, and Early Number Concepts; MABC-two Total, Manual Dexterity, and Balance; and the Phonological Awareness subtest of the Test of Preschool Early Literacy (TOPEL) [48]. Analyses also revealed significant group × sex interactions for the CTOPP-2 Rapid Symbolic Naming, Conners EC-P Social Functioning, and ERC Emotion Regulation, as well as a significant group × zSES interaction for MABC-two Aiming and Communicable. VPT boys had lower CTOPP-two Rapid Symbolic Naming scores than FT boys (p = 0.002; ES = −i.eighteen). Compared to FT girls, VPT girls had higher Conners EC-P Social Operation (i.due east., worse social functioning) (p < 0.001, ES = 1.42) and lower ERC Emotion Regulation (p < 0.001, ES = i.20).
Main furnishings for sex activity and zSES were significant in analyses of several of the measures (information not shown). Boys had higher scores than girls on DAS-Ii Recall of Digits-Forward and lower scores on the MABC-ii Total. Higher zSES was associated with higher scores on DAS-2 Spatial Ability and TOPEL Print Cognition and with lower ratings of behavior problems on the Conners EC-P Global Alphabetize and Inattention/Hyperactivity; Brief GEC, Inhibitory Self-Command, Flexibility, and Emergent Metacognition; and ERC Lability/Negativity.
Fifty-fifty when adjusting for the DAS-Two GCA, differences remained significant for MABC-2 Total (p = 0.002, ES = 0.74) and Manual Dexterity (p = 0.015, ES = 0.60). Consequent with results from analyses that did non adjust for the DAS-II GCA, these analyses also revealed significant grouping × sexual activity interactions for Conners EC-P Social Functioning (p < 0.001) and ERC Emotion Regulation (p = 0.003). VPT girls had significantly higher ratings of bug than FT girls on Conners EC-P Social Performance (p < 0.001, ES = 1.21) and lower ratings on ERC Emotion Regulation (p = 0.003, ES = −one.11). Group differences in these measures were not significant for boys.
In the GEE analysis that included the measure from each domain with the largest ES as predictors of group membership (DAS-2 GCA, Recall of Digits-Forward, and Early Number Concepts; MABC-2 Total; and Brief-P Emergent Metacognition Index), the MABC-2 Total was the only measure significantly associated with grouping independently of the other predictors, beta (standard fault) = 0.35 (0.14), p = 0.011.
3.2. Group Differences in Rates of Deficits
Similar to results from mixed model analyses, odds of deficits were significantly higher for the VPT group than for the FT grouping on well-nigh of the measures (see Tabular array 4). Rates of deficits on the operation tests for which group differences were significant ranged from eighteen% to 74% for the VPT grouping compared to 0% to 26% for the FT group. A significantly higher proportion of the VPT group besides had deficits on Conners EC-P Social Functioning, Brief-P GEC, Inhibitory Self-Control, and Emergent Metacognition. Rates of deficits on these measures ranged from 32% to 57% for the VPT group compared to 3% to 16% for the FT group. Deficits in multiple readiness measures were also significantly higher in the VPT group compared to the FT group (83% versus 32%).
3.3. Readiness Profiles
Model fit statistics were improve for the 4- and v-class models relative to the 1-, 2- and 3-grade models (Table v), thus the 1- to 3-form models were rejected. The 5-class model compared less favorably to the iv-course model based on Entropy and BIC. The 4-class model, shown in Effigy i, was selected as it was more than interpretable and resulted in lower BIC indices and higher entropy relative to the 5-grade model.
The 37 children assigned to latent class ane had the best readiness outcomes, with scores on performance tests and behavior ratings falling well inside the boilerplate range. Merely 8 VPT children were in this class (22% of class). Scores on all performance tests were lower for the 20 participants in latent class 2 than for those in grade ane. Fourteen of these children (70%) were from the VPT group. Although latent class 2 participants had higher test scores than those in latent classes 3 or four, they had more behavior bug than the xiv children in latent class three, of whom 13 (93%) were from the VPT group. The four participants assigned to latent grade iv, all from the VPT grouping, had the worst outcomes on all readiness measures.
Although group separation is optimized in LCA, support for these interpretations was provided by pairwise comparisons of readiness scores for the four latent classes. Specifically: (1) each of the four latent classes differed significantly from the other classes on the DAS-Two Verbal and Spatial Ability and Conners EC-P Anxiety; (2) grade 1 had significantly higher test scores than classes two and three on DAS-2 Exact, Nonverbal, and Spatial composites, DAS-II Recalling of Digits-Forward, TOPEL Print Noesis and Phonological Sensation, DAS-Two Early Number Concepts, and MABC-ii, as well as significantly lower ratings on Conners EP-C Anxiety; and (3) class 2 had higher scores than class 3 on TOPEL Phonological Awareness but significantly college ratings of behavior bug on Conners EC-P Inattention/Hyperactivity and Anxiety, BRIEF-P GEC, and ERC Lability/Negativity. The four latent classes as well differed significantly in group membership (significantly college proportion of the FT group in form 1 compared to the class three), zSES (significantly college in class 1 compared to class 2), and GA (significantly college in class 1 compared to classes one, 2, and 3).
4. Word
This written report compared 4-year-one-time VPT children to FT controls on a wide range of measures of schoolhouse readiness to identify measures of readiness on which the VPT grouping had the greatest difficulty and to examine variations in readiness issues. The VPT group performed most poorly relative to the FT group on tests of spatial ability, exact working memory, motor performance, phonological processing, and number skills. Problems in psychosocial functioning that distinguished the VPT group from FT controls were in areas of executive office, and, at least for females, in emotion regulation and social performance, although the ESs corresponding to these differences were not equally large equally those for group differences on the aforementioned functioning measures. Group differences in rates of deficits were also the about pronounced for the performance measures. For example, nearly one-third of VPT children had deficits in global cognition compared to none of the FT preschoolers. Deficits like to those observed in this study are reported in previous studies of both VPT preschoolers [4,10,11,17,22,52] and school-age VPT children [16,33,37,53,54,55,56,57]. The present study adds to this literature past assessing the variability of harm displayed by VPT preschoolers across a range of readiness measures.
Although differences between the VPT and FT group were largely independent of sexual activity and zSES in this and other studies [xviii], deficits in CTOPP-two Rapid Symbolic Naming were plant only for VPT boys, and more caregiver-rated problems on the Conners EC-P Social Operation and weakness in ERC Emotion Regulation were axiomatic but for VPT girls. Despite inconsistencies in reports of sex activity-related differences in the consequences of VPT birth, some previous enquiry supports the possibility of more pronounced effects for males than for females [58]. Nosotros are unaware of testify to suggest that females are more vulnerable than males to adverse socioemotional consequences of VPT birth. Potential explanations include gender differences in early on socialization processes [59] or gender-related biases in parent ratings of socioemotional functioning [60]. We besides plant that differences in favor of the FT group on motor skills, as assessed by the MABC-2 Total, were more pronounced amidst children with lower zSES. The moderating issue of SES on group differences in motor ability is like to findings suggesting more than adverse effects of maternal insensitivity on academic accomplishment for low birth weight children compared to normal nativity weight youth [61], and raises the possibility that readiness issues in VPT preschoolers may be exacerbated past ecology disadvantage. The latter finding is too consistent with bear witness for a greater intervention effect on motor issue for VPT children at higher social risk [62]. Even so, support from our study for sexual activity- and zSES-related differences in the effects of VPT nativity were limited to these measures. In view of the lack of more consequent evidence for these factors equally moderators of VPT outcomes from this report or by research, caution is brash in interpreting these findings pending larger-scale studies of VPT preschoolers' school readiness.
Near of the group differences in school readiness were non pregnant when adjusting for the DAS-II GCA, suggesting that problems in school readiness for many VPT preschoolers are associated with weaknesses in global cognitive ability. The finding of higher rates of multiple deficits in the VPT preschoolers compared to the FT group also points to pervasive problems in readiness in many VPT children. The results confirm previous findings of pervasive developmental deficits in VPT cohorts, as well equally observations of associations between cognitive weaknesses and behavior bug in these children [28,29].
Yet, other findings from this study indicate that some children may have more selective problems in readiness. To begin with, even controlling for the DAS-II GCA, the VPT group relative to FT controls performed more poorly on measures of motor skills, and VPT girls were rated past caregivers as having more problems in social functioning and lower levels of emotion regulation relative to FT girls. Second, in GEE analysis that included a ready of the most discriminating readiness measures from each of the 5 domains as predictors of group membership, motor ability discriminated the groups independently of other measures of readiness. These results underscore motor skills equally a critical domain in cess of readiness [4,10,63,64], and propose that, at least for females, some socio-emotional aspects of school readiness may be affected independently of their cerebral competencies.
Third, findings from the LCA provided support for four individual patterns of readiness competencies. Classes 1 and 4, respectively, identified preschoolers with either strengths or weaknesses beyond all readiness domains. The other two classes were characterized past scores on performance tests that fell between those of classes 1 and four merely differed in their profiles of relative strengths and weaknesses. Relative to the children assigned to form 3, those in class 2 performed at somewhat higher levels on tests of cognitive and motor skills but also had higher caregiver ratings of behavior problems. These findings are consistent with research suggesting that some VPT children display historic period-typical outcomes beyond multiple developmental domains, while others have either selective or generalized impairments [21,22,25,26,27,31,41]. Inquiry examining readiness profiles in community samples of kindergarteners or kickoff graders reveals similar findings [ix,23,24]. Every bit was evident in the present sample, these studies identified subgroups of children with uniformly positive or negative outcomes across readiness domains, too as subgroups showing dissociations betwixt cognitive and behavioral aspects of readiness. Evidence for latent classes comprising both VPT and FT preschoolers (i.eastward., classes 1–iii) is likewise consistent with results from prior LCAs that have classified children from both these groups into the same behavioral profiles [25,65].
These findings need to be considered in the context of several report limitations. First, because of the numerous school readiness measures examined, the relatively small sample, and the lack of correction for multiple comparisons, findings are viewed more as hypothesis-generating than as hypothesis-driven. The results likely depended on the measures administered and on sample characteristics. Assessments were comprehensive, but some aspects of readiness, such every bit children'south health condition, physical development, and temperament, were not evaluated. The nowadays study also did not consider the level of support provided past families and communities equally additional contributors to school readiness [8,9].
Data from all children who participated in the study were included in the analysis, and the VPT group was similar to other VPT cohorts in terms of mean GA and neonatal complications [31]. Nonetheless, recruitment did not ensure representativeness relative to the broader VPT population. Findings may be more than informative of the nature of readiness problems in preschoolers capable of engaging in testing than of the outcomes of VPT nascency more generally. Additionally, FT preschoolers were recruited from a pool of families that had volunteered for research and that had higher hateful zSES than the families of VPT preschoolers. Although zSES was controlled in analyses, the VPT and FT groups were not matched on background characteristics and it is unclear how representative the FT group was of the broader regional customs of preschool children.
Prove from LCA of distinct profiles of readiness is as well preliminary and requires replication with larger samples. Samples larger than the present ane are ordinarily recommended in conducting LCA, though smaller samples may be needed in LCA involving more and higher-quality indicators [66,67]. The substantial number of readiness measures assessed in this report may thus have contributed to the reasonable fit indices obtained by the nowadays LCA. The four profiles of readiness characteristics identified by the LCA are besides similar to those reported in previous studies of older VPT children. Boosted studies are nonetheless needed to further our understanding of the nature of individual differences in readiness amid VPT preschoolers. Examination of associations of profile types with subsequent bookish progress and with medical and ecology risk factors would too be useful, as has been conducted in slightly older samples of VPT children [9,26,27].
Despite these limitations, the results have important clinical implications for assessing, monitoring, and treating readiness difficulties in VPT preschoolers. The sensitivity of methods for identifying readiness problems would exist enhanced past assessing the aspects of readiness near likely to be affected by VPT nascency. Based on the nowadays findings, these domains include functioning on tests of spatial and nonverbal knowledge, executive function, motor skills, phonological processing, and numeracy. Findings besides support the inclusion of caregiver ratings of dysexecutive behavior and bug in social functioning and emotion regulation. Readiness problems may be manifest in global weaknesses in test performance and psychosocial aligning, or may manifest as milder or more selective deficits. Inclusion of tests of motor skills and measures of social functioning and emotion regulation appears particularly important in designing assessments of readiness, given the evidence for weaknesses in these areas that are independent of global cognitive ability.
Weaknesses in multiple readiness measures in seventy% of the VPT group underscore the disquisitional need for universal monitoring of readiness skills in this population before school entry [5,ten,15,68]. Beyond surveillance, results of monitoring assessments allow efficient and specific targeting of interventions to address aspects of readiness most impaired in VPT preschoolers. These approaches might entail efforts to remediate skill deficiencies or to adapt for them in ways that minimize disruptions to the learning procedure. The need for broader-based preschool interventions is underscored by VPT preschoolers' difficulties in multiple readiness domains, along with the potential negative consequences of delayed readiness on longer-term educational and employment outcomes [4,5,x,nineteen]. Exemplary interventions are programs that involve both school- and family-based activities and that accost children's socioemotional performance, also equally their specific weaknesses in cognitive, motor, and early literacy and numeracy skills [thirteen,19]. As like proportions of the VPT and FT groups were enrolled in preschool, the nowadays findings align with previous evidence suggesting that preschool attendance alone, absent interventions directed to the specific needs of VPT children, is unlikely to narrow the "preschool readiness gap" [69].
Follow-upward of the present sample into early school age would be informative in investigating readiness measures and profiles equally predictors of school-age achievement. Although associations of readiness measures with after achievement in both VPT preschoolers and larger community samples are well-documented [4,xix,23,24], further research is required to place the best predictors. Evidence that certain measures of readiness are highly predictive of subsequent achievement would contend for their inclusion in preschool assessments. A ameliorate agreement of the sources of readiness problems volition also require more enquiry on the neonatal, early developmental, and ecology factors associated with these deficits. The present findings are consequent with previous research in documenting associations of greater sociodemographic disadvantage with difficulties on several of the readiness measures [5,17,63,70]. However, more accent on the relation of readiness to other, potentially modifiable, characteristics of the family or preschool setting would take greater utility in developing interventions.
5. Conclusions
The findings from this study suggest that effects of VPT nativity on schoolhouse readiness are virtually probable to be manifest in tests of spatial, nonverbal, and motor skills, executive function, phonological processing, and early number knowledge. Agin effects on behavioral aspects of readiness, such as behavioral manifestations of executive deficits and problems in social functioning and emotion regulation, are also evident, merely are less pronounced or related to sexual practice. Variability in the types of readiness problems displayed by VPT preschoolers is supported by findings of independent effects of VPT birth on global cognition and motor skills and by variable profiles of readiness skills in the VPT group. These results will assistance guide the development of more than constructive approaches to identify those VPT children in need of more intensive early on educational interventions and may also help target those interventions. Efforts to replicate the present findings with larger and more representative samples are critical in refining methods for identifying private variations in readiness and informing interventions targeted to specific profiles of strengths and weaknesses.
Author Contributions
Conceptualization, H.G.T., Northward.L.Yard., M.L.North., A.d.Southward.; methodology, H.Thousand.T., Northward.L.Yard., M.L.N., A.d.S.; formal analysis, D.1000.V., R.B., T.A.B., Due south.U.; investigation, M.L.Northward., A.d.South., T.A.B.; data curation, T.A.B., R.B.; writing—original draft preparation, H.One thousand.T., D.1000.V., R.B.; writing—review and editing, H.G.T., D.Yard.5., M.L.Northward., R.B., T.A.B., A.d.Southward., S.U., N.50.M.; supervision, H.One thousand.T., N.Fifty.M.; project administration, H.One thousand.T., N.L.M.; funding acquisition, H.Grand.T., N.50.Chiliad. All authors accept read and agreed to the published version of the manuscript.
Funding
This research was funded by the Abigail Wexner Enquiry Institute at Nationwide Children's Hospital, cost center 40310-0008.
Institutional Review Board Statement
The report was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Lath of Nationwide Children's Hospital (protocol IRB18-00446, appointment of blessing August 2018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the written report.
Information Availability Statement
The data presented in this study are available from the corresponding author subject to approval by the investigators, institutional review, and an approved data use understanding. The data are not still publicly available pending sufficient fourth dimension for the investigators to study on the findings.
Acknowledgments
The authors capeesh the assistance of Kerry Orton and Stephanie Burkhardt in projection coordination and of examiners Sandra Glazer, Hanan Guzman, Kaleigh Hague, Brianna Laney, Julia Newton, Katelyn Keener, Megan Lightfoot, Ashley Widmayer, Gabrielle Moots, Caitlin Kjeldsen, Lindsey Pietruszewski, and Brianna Sowers. We acknowledge Joseph Rausch, in the Center for Biobehavioral Wellness at Nationwide Children's Hospital and Nori Minich in the Department of Pediatrics at Case Western Reserve University for statistical consultation. We besides acknowledge Sasha Key, of Vanderbilt University for creating a estimator-based version of the Zoo Game Go No Go Examination for this study and as a collaborator on the larger schoolhouse readiness projection. We are also grateful to the children and families who participated in the study.
Conflicts of Interest
The authors declare no conflict of involvement.
References
- Johnson, S.; Wolke, D.; Hennessy, E.; Marlow, N. Educational Outcomes in Extremely Preterm Children: Neuropsychological Correlates and Predictors of Attainment. Dev. Neuropsychol. 2011, 36, 74–95. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, 5.E.; Clark, C.A.; Liberty, K.; Champion, P.R.; Wilson, 1000.; Woodward, L.J. Early schoolhouse-based learning difficulties in children born very preterm. Early Hum. Dev. 2009, 85, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Aylward, Yard.P. Neurodevelopmental outcomes of infants born prematurely. J. Dev. Behav. Pediatr. 2014, 35, 394–407. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, V.Eastward.; Bora, South.; Austin, N.C.; Levin, K.J.; Woodward, 50.J. Identifying very preterm children at educational risk using a school readiness framework. Pediatrics 2014, 134, e825–e832. [Google Scholar] [CrossRef]
- Shah, P.E.; Kaciroti, N.; Richards, B.; Lumeng, J.C. Gestational age and kindergarten school readiness in a national sample of preterm infants. J. Pediatr. 2016, 178, 61–67. [Google Scholar] [CrossRef]
- Taylor, H.G.; Klein, North.; Anselmo, K.Grand.; Minich, Northward.; Espy, K.A.; Hack, M. Learning problems in kindergarten students with extremely preterm birth. Arch. Pediatr. Adolesc. Med. 2011, 165, 819–825. [Google Scholar] [CrossRef]
- High, P.C.; The Pediatrics Committee on Early Childhood, Adoption and Dependent Intendance and Council on Schoolhouse Health. School readiness. Pediatrics 2008, 121, e1008–e1015. [Google Scholar] [CrossRef]
- Williams, P.G.; Lerner, Thousand.A.; Quango On Early Childhood; Quango On School Wellness; Sells, J.; Alderman, Southward.L.; Hashikawa, A.; Mendelsohn, M.A.; Mc Fadden, T.; Navsaria, D.; et al. School readiness. Pediatrics 2019, 144, e20191766. [Google Scholar] [CrossRef]
- Pan, Q.; Trang, K.T.; Love, H.R.; Templin, J. School readiness profiles and growth in bookish achievement. Forepart. Educ. 2019, iv, 127. [Google Scholar] [CrossRef]
- Roberts, K.; Lim, J.; Doyle, L.Westward.; Anderson, P.J. High rates of school readiness difficulties at 5 years of historic period in very preterm infants compared with term controls. J. Dev. Behav. Pediatr. 2011, 32, 117–124. [Google Scholar] [CrossRef]
- Baron, I.S.; Erickson, K.; Ahronovich, Thousand.D.; Bakery, R.; Litman, F.R. Neuropsychological and behavioral outcomes of extremely depression birth weight at age iii. Dev. Neuropsychol. 2011, 36, 5–21. [Google Scholar] [CrossRef]
- Baron, I.S.; Kerns, Thousand.A.; Muller, U.; Ahronovich, Grand.D.; Litman, F.R. Executive functions in extremely low birth weight and late-preterm preschoolers: Effects on working retentivity and response inhibition. Child Neuropsychol. 2012, xviii, 586–599. [Google Scholar] [CrossRef]
- Blair, C.; Raver, C.C. Schoolhouse readiness and self-regulation: A developmental psychobiological approach. Annu. Rev. Psychol. 2015, 66, 711–731. [Google Scholar] [CrossRef]
- Clark, C.A.C.; Pritchard, V.E.; Woodward, L.J. Preschool executive functioning abilities predict early on mathematics accomplishment. Dev. Psychol. 2010, 46, 1176–1191. [Google Scholar] [CrossRef]
- Foster-Cohen, S.H.; Friesen, M.D.; Champion, P.R.; Woodward, L.J. Loftier prevalence/low severity language delay in preschool children born very preterm. J. Dev. Behav. Pediatr. 2010, 31, 658–667. [Google Scholar] [CrossRef]
- Hasler, H.G.; Akshoomoff, N. Mathematics ability and related skills in preschoolers born very preterm. Kid Neuropsychol. 2019, 25, 162–178. [Google Scholar] [CrossRef]
- Jones, K.1000.; Champion, P.R.; Woodward, L.J. Social competence of preschool children born very preterm. Early Hum. Dev. 2013, 89, 795–802. [Google Scholar] [CrossRef]
- Taylor, H.K.; Klein, N.; Espy, Chiliad.A.; Schluchter, Thousand.; Minich, N.; Stilp, R.; Hack, M. Furnishings of farthermost prematurity and kindergarten neuropsychological skills on early bookish progress. Neuropsychology 2018, 32, 809–821. [Google Scholar] [CrossRef]
- Woodward, Fifty.J.; Lu, Z.; Morris, A.; Healey, D. Self regulatory skills during early babyhood are associated with later mental health and educational accomplishment in very preterm and typically developing children. Clin. Neuropsychol. 2017, 31, 404–422. [Google Scholar] [CrossRef]
- Anderson, P.J. Neuropsychological outcomes of children born very preterm. Semin. Fetal Neonatal Med. 2014, 19, 90–96. [Google Scholar] [CrossRef]
- Anderson, P.J.; Doyle, L.W. Cognitive and educational deficits in children born extremely preterm. Semin. Perinatol. 2008, 32, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Woodward, L.J.; Moor, S.; Hood, K.One thousand.; Champion, P.R.; Foster-Cohen, South.; Inder, T.E.; Austin, Due north.C. Very preterm children show impairments across multiple neurodevelopmental domains past age four years. Arch. Dis. Child Fetal Neonatal Ed. 2009, 94, F339–F344. [Google Scholar] [CrossRef]
- Hair, E.; Halle, T.; Terry-Humen, E.; Lavelle, B.; Calkins, J. Children'southward schoolhouse readiness in the ECLS-M: Predictions to academic, health, and social outcomes in first grade. Early Child. Res. Q. 2006, 21, 431–454. [Google Scholar] [CrossRef]
- Konold, T.R.; Pianta, R.C. Empirically-derived, person-oriented patterns of school readiness in typically-developing children: Clarification and prediction to first-class accomplishment. Appl. Dev. Sci. 2005, 9, 174–187. [Google Scholar] [CrossRef]
- Burnett, A.C.; Youssef, G.; Anderson, P.J.; Duff, J.; Doyle, 50.W.; Cheong, J.L.Y.; Victorian Infant Collaborative Study Group. Exploring the "preterm behavioral phenotype" in children built-in extremely preterm. J. Dev. Behav. Pediatr. 2019, 40, 200–207. [Google Scholar] [CrossRef]
- Twilhaar, E.S.; Pierrat, V.; Marchand-Martin, L.; Benhammou, 5.; Kaminski, 1000.; Ancel, P.Y. Profiles of functioning in five.5-year-old very preterm born children in france: The EPIPAGE-2 report. J. Am. Acad. Child Adolesc. Psychiatry 2021. [Google Scholar] [CrossRef]
- Lean, R.E.; Lessov-Shlaggar, C.N.; Gerstein, E.D.; Smyser, T.A.; Paul, R.A.; Smyser, C.D.; Rogers, C.E. Maternal and family factors differentiate profiles of psychiatric impairments in very preterm children at historic period 5-years. J. Kid Psychol. Psychiatry 2020, 61, 157–166. [Google Scholar] [CrossRef]
- Alduncin, N.; Huffman, L.C.; Feldman, H.M.; Loe, I.M. Executive part is associated with social competence in preschool-aged children built-in preterm or full term. Early Hum. Dev. 2014, ninety, 299–306. [Google Scholar] [CrossRef]
- Delobel-Ayoub, M.; Arnaud, C.; White-Koning, K.; Casper, C.; Pierrat, V.; Garel, M.; Burguet, A.; Roze, J.C.; Matis, J.; Picaud, J.C.; et al. Behavioral issues and cognitive performance at 5 years of historic period afterwards very preterm birth: The EPIPAGE Written report. Pediatrics 2009, 123, 1485–1492. [Google Scholar] [CrossRef]
- Witt, A.; Theurel, A.; Tolsa, C.B.; Lejeune, F.; Fernandes, Fifty.; de Jonge, L.; Monnier, M.; Bickle Graz, M.; Barisnikov, K.; Gentaz, Eastward.; et al. Emotional and effortful control abilities in 42-month-old very preterm and full-term children. Early on Hum. Dev. 2014, 90, 565–569. [Google Scholar] [CrossRef]
- De Silva, A.; Neel, Yard.L.; Maitre, North.; Busch, T.; Taylor, H.K. Resilience and vulnerability in very preterm 4-year-olds. Clin. Neuropsychol. 2021, 35, 904–924. [Google Scholar] [CrossRef]
- Neel, M.L.; de Silva, A.; Taylor, H.G.; Benninger, K.; Busch, T.; Hone, E.; Moore-Clingenpeel, One thousand.; Pietruszewski, L.; Maitre, N.L. Exceeding expectations later on perinatal risks for poor development: Associations in term- and preterm-built-in preschoolers. J. Perinatol. 2021. [Google Scholar] [CrossRef]
- Orchinik, L.J.; Taylor, H.G.; Espy, K.A.; Minich, North.; Klein, N.; Sheffield, T.; Hack, M. Cerebral outcomes for extremely preterm/extremely low birth weight children in kindergarten. J. Int. Neuropsychol. Soc. 2011, 17, 1067–1079. [Google Scholar] [CrossRef]
- Mohammad, One thousand.; Scott, J.N.; Leijser, 50.M.; Zein, H.; Afifi, J.; Piedboeuf, B.; de Vries, L.S.; van Wezel-Meijler, G.; Lee, Due south.K.; Shah, P.Southward. Consensus Arroyo for Standardizing the Screening and Nomenclature of Preterm Brain Injury Diagnosed with Cranial Ultrasound: A Canadian Perspective. Front. Pediatr. 2021, 9, 618236. [Google Scholar] [CrossRef]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A written report of infants with nascence weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar] [CrossRef]
- Conners, C.Grand. Conners Early on Childhood.; Multi-Health Systems, Inc.: Toronto, ON, Canada, 2009. [Google Scholar]
- Johnson, Southward.; Marlow, Due north. Preterm birth and childhood psychiatric disorders. Pediatr. Res. 2011, 69, 11R–18R. [Google Scholar] [CrossRef]
- Lamm, C.; Walker, O.L.; Degnan, K.A.; Henderson, H.A.; Pino, D.S.; McDermott, J.Grand.; Trick, N.A. Cognitive command moderates early childhood temperament in predicting social behavior in 7-year-old children: An ERP study. Dev. Sci. 2012, 17, 667–681. [Google Scholar] [CrossRef]
- Shields, A.; Cicchetti, D. Emotion regulation amongst school-age children: The evolution and validation of a new criterion Q-sort calibration. Dev. Psychol. 1997, 33, 906–916. [Google Scholar] [CrossRef]
- Griffiths, A.; Morgan, P.; Anderson, P.J.; Doyle, L.W.; Lee, K.J.; Spittle, A.J. Predictive value of the movement assessment bombardment for children—Second Edition at 4 years, for motor impairment at 8 years in children born preterm. Dev. Med. Child Neurol. 2017, 59, 490–496. [Google Scholar] [CrossRef]
- Taylor, H.G.; Minich, N.; Schluchter, M.; Espy, Grand.A.; Klein, North. Resilience in Extremely preterm/extremely depression birth weight kindergarten children. J. Int. Neuropsychol. Soc. 2019, 25, 362–374. [Google Scholar] [CrossRef]
- Wiley, C.P.; Wedeking, T.; Galindo, A.One thousand. Test review: C.Yard. Test Review: CK Conners. Conners early childhood manual. J. Psychoeduc. Assess. 2013, 31, 606–610. [Google Scholar] [CrossRef]
- Zelazo, P.D.; Muller, U.; Frye, D.; Marcovitch, S.; Argitis, Thousand.; Boseovski, J.; Chiang, J.K.; Hongwanishkul, D.; Schuster, B.V.; Sutherland, A. The development of executive function in early babyhood. Monogr. Soc. Res. Child Dev. 2003, 68, vii-137. [Google Scholar] [CrossRef] [PubMed]
- Elliot, C.D. Differential Ability Scales, 2nd ed.; Harcourt Assessment: San Antonio, TX, The states, 2007. [Google Scholar]
- Casaletto, K.B.; Umlauf, A.; Beaumont, J.; Gershon, R.; Slotkin, J.; Akshoomoff, Due north.; Heaton, R.Grand. Demographically corrected normative standards for the English version of the NIH Toolbox Cognition Battery. J. Int. Neuropsychol. Soc. 2015, 21, 378–391. [Google Scholar] [CrossRef] [PubMed]
- Wagner, R.; Torgensen, J.; Rashotte, C.; Pearson, N. Comprehensive Exam of Phonological Processing, 2nd ed.; PRO-ED: Austin, TX, United states, 2013. [Google Scholar]
- Henderson, Due south.Eastward.; Sugden, D.A.; Barnett, A. Move Assessment Battery for Children (Movement ABC-2): Examiner's Manual, 2nd ed.; Harcourt Assessment: London, UK, 2007. [Google Scholar]
- Lonigan, C.J.; Wagner, R.K.; Torgensen, J.K.; Rashotte, C.A. TOPEL: Test of Preschool Early Literacy; Pro-Ed: Austin, TX, USA, 2007. [Google Scholar]
- Wilson, S.B.; Lonigan, C.J. An evaluation of two emergent literacy screening tools for preschool children. Ann. Dyslexia 2009, 59, 115–131. [Google Scholar] [CrossRef] [PubMed]
- Gioia, K.A.; Espy, K.A.; Esquith, P.G. BRIEF-P: Behavior Rating Inventory of Executive Function—Preschool Version; Psychological Cess Resource: Lutz, FL, USA, 2003. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Pitchford, N.; Johnson, South.; Scerif, Grand.; Marlow, North. Early indications of delayed cognitive evolution in preschool children born very preterm: Evidence from domain-general and domain-specific tasks. Baby Child Dev. 2011, twenty, 400–422. [Google Scholar] [CrossRef]
- Businesswoman, I.South.; Brandt, J.; Ahronovich, Yard.D.; Baker, R.; Erickson, One thousand.; Litman, F.R. Selective arrears in spatial location memory in extremely low nativity weight children at age six: The PETIT study. Kid Neuropsychol. 2012, xviii, 299–311. [Google Scholar] [CrossRef]
- Larson, J.C.G.; Barson, I.S.; Erickson, K.; Ahronovich, M.D.; Baker, R.; Litman, F.R. Neuromotor outcomes at school age after extremely low birth weight: Early on detection of subtle signs. Neuropsychology 2011, 25, 66–75. [Google Scholar] [CrossRef]
- Scott, M.N.; Taylor, H.K.; Fristad, One thousand.A.; Klein, N.; Espy, K.A.; Minich, Northward.; Hack, One thousand. Beliefs disorders in extremely preterm/extremely low nativity weight children in kindergarten. J. Dev. Behav. Pediatr. 2012, 33, 202–213. [Google Scholar] [CrossRef]
- Taylor, H.Thou. Neurodevelopmental origins of social competence in very preterm children. Semin. Fetal Neonatal. Med. 2020, 25, 101108. [Google Scholar] [CrossRef]
- Taylor, H.K.; Clark, C.A.C. Executive part in children born preterm: Run a risk factors and implications for event. Semin. Perinatol. 2016, forty, 520–529. [Google Scholar] [CrossRef]
- O'Driscoll, D.N.; McGovern, Grand.; Greene, C.Yard.; Molloy, E.J. Gender disparities in preterm neonatal outcomes. Acta Paediatr. 2018, 107, 1494–1499. [Google Scholar] [CrossRef]
- Underwood, M.K.; Galen, B.R.; Paquette, J.A. Peak ten challenges for understanding gender and aggression in children: Why tin't we all just get along? Soc. Dev. 2001, 10, 248–266. [Google Scholar] [CrossRef]
- Najman, J.Chiliad.; Williams, G.M.; Nikles, J.; Spence, Due south.; Bor, W.; O'Callaghan, M.; Le Brocque, R.; Andersen, One thousand.J.; Shuttlewood, K.J. Bias influencing maternal reports of child behaviour and emotional state. Soc. Psychiatry Psychiatr. Epidemiol. 2001, 36, 186–194. [Google Scholar] [CrossRef]
- Jaekel, J.; Pluess, Yard.; Belsky, J.; Wolke, D. Effects of maternal sensitivity on low birth weight children's academic achievement: A exam of differential susceptibility versus diathesis stress. J. Child Psychol. Psychiatry 2015, 56, 693–701. [Google Scholar] [CrossRef]
- Spittle, A.J.; Treyvaud, Grand.; Lee, K.J.; Anderson, P.J.; Doyle, L.Due west. The role of social risk in an early preventative care programme for infants born very preterm: A randomized controlled trial. Dev. Med. Child Neurol. 2018, threescore, 54–62. [Google Scholar] [CrossRef]
- Benavente-Fernandez, I.; Synnes, A.; Grunau, R.Due east.; Chau, V.; Ramraj, C.; Drinking glass, T.; Cayam-Rand, D.; Siddiqi, A.; Miller, S.P. Association of socioeconomic condition and encephalon injury with neurodevelopmental outcomes of very preterm children. JAMA Netw. Open 2019, two, e192914. [Google Scholar] [CrossRef]
- Duncan, A.F.; Bann, C.G.; Maitre, N.L.; Peralta-Carcelen, Yard.; Hintz, S.R.; Eunice Kennedy Shriver National Found of Child Health; Development Neonatal Research Network. Hand function at 18–22 months is associated with schoolhouse-age transmission dexterity and motor performance in children born extremely preterm. J. Pediatr. 2020, 225, 51–57. [Google Scholar] [CrossRef]
- Johnson, S.; Waheed, G.; Manktelow, B.N.; Field, D.J.; Marlow, Due north.; Draper, Due east.South.; Boyle, E.Thousand. Differentiating the preterm phenotype: Distinct profiles of cerebral and behavioral development following late and moderately preterm birth. J. Pediatr. 2018, 193, 85–92. [Google Scholar] [CrossRef]
- Weller, B.East.; Bowen, North.K.; Faubert, S.J. Latent form assay: A guide to best exercise. J. Black Psychol. 2020, 46, 287–311. [Google Scholar] [CrossRef]
- Wurpts, I.C.; Geiser, C. Is adding more indicators to a latent class analysis benign or detrimental? Results of a monte-carlo study. Front. Psychol. 2014, v, 920. [Google Scholar] [CrossRef] [PubMed]
- Chung, P.J.; Opipari, V.P.; Koolwijk, I. Executive function and extremely preterm children. Pediatr. Res. 2017, 82, 565–566. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Claessens, A.; Msall, Thou.E. Prematurity and school readiness in a nationally representative sample of Australian children: Does typically occurring preschool moderate the relationship? Early on Hum. Dev. 2014, 90, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Doyle, Fifty.W.; Cheong, J.L.; Burnett, A.; Roberts, Grand.; Lee, Thou.J.; Anderson, P.J.; Victorian Infant Collaborative Study, 1000. Biological and social influences on outcomes of extreme-preterm/low-birth weight adolescents. Pediatrics 2015, 136, e1513–e1520. [Google Scholar] [CrossRef]
Figure ane. Latent class differences in hateful z scores for readiness measures.
Figure 1. Latent grade differences in mean z scores for readiness measures.
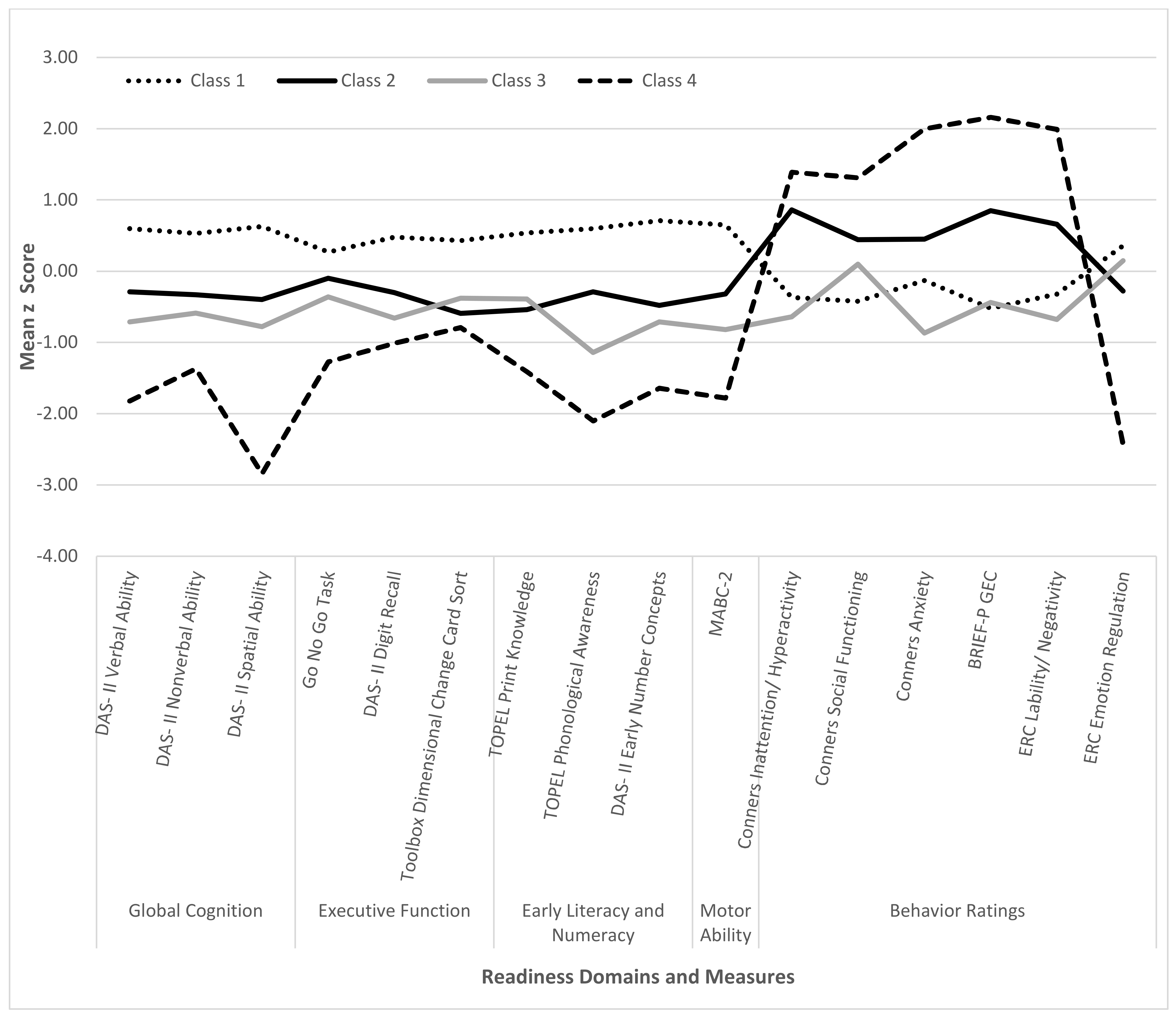
Table one. Sample characteristics.
Table ane. Sample characteristics.
| Characteristic | Group | |
|---|---|---|
| VPT (n = 53) | FT (n = 38) | |
| Neonatal and early developmental status: | ||
| Child age, mean (SD) | 4.7 (0.29) | 4.vi (0.29) |
| Gestational age, mean in weeks (SD, range) a,b | 27.iii (1.9, 23–thirty) | 39.1 (1.i, 37–41) |
| Birth weight in grams, mean (SD, range) a,b | 944 (270, 369–1644) | 3249 (435, 2325–4167) |
| Multiple birth c, n (%) | ten (45) | ii (11) |
| Medical complications | ||
| Class III-IVH or PVHI d, north (%) | half-dozen (11.32) | - |
| Periventricular leukomalacia e, n (%) | 10 (18.ix) | - |
| Bronchopulmonary dysplasia requiring home oxygen, northward (%) | 16 (30.2) | - |
| Intrauterine growth brake (IUGR), n (%) | vii (13.2) | - |
| Culture-positive sepsis, n (%) | 14 (26.4) | - |
| Necrotizing enterocolitis (NEC) f, due north (%) | half-dozen (11.iii) | - |
| Retinopathy of prematurity (ROP) requiring light amplification by stimulated emission of radiation surgery, n (%) | 4 (7.v) | - |
| Family demographic characteristics: | ||
| Kid sex: male, n (%) | 27 (50.9) | eighteen (47.4) |
| Kid race: | ||
| White, n (%) | 35 (66) | 28 (73.vii) |
| Black/African American, northward (%) | 10 (18.9) | three (seven.nine) |
| Asian, due north (%) | 1 (1.9) | 1 (2.vi) |
| More than than one race, north (%) | vii (13.ii) | half-dozen (15.8) |
| Child enrolled in preschool, n (%) | 46 (86.8) | 32 (84.2) |
| zSES Blended, mean (SD) a | −0.25 (0.73) | 0.35 (0.59) |
Table ii. Readiness measures.
Table two. Readiness measures.
| Domain/Measure | Reference | Description | Score |
|---|---|---|---|
| Global cognitive ability (DAS-II): | [44] | Standard Scores | |
| DAS-2 Full general Conceptual Power | Global ability composite | ||
| DAS-II Verbal Power | Verbal comprehension and naming | ||
| DAS-2 Nonverbal Ability | Nonverbal reasoning | ||
| DAS-Ii Spatial Ability | Perceptual motor skills | ||
| Executive function and processing speed: | |||
| NIH Toolbox Dimensional Modify Bill of fare Sort | [45] | Cognitive power/rule shifting | T-score a |
| DAS-Ii Recall of Digits—Forward | [44] | Verbal working memory | T-score |
| Zoo Game Go No Go Task b | [38] | Attention and inhibition | Proportion right |
| CTOPP-2 Rapid Symbolic Naming c | [46] | Speed of naming | Standard score |
| Motor skills (MABC-2): | [47] | Scaled scores | |
| Total | Composite of motor skills | ||
| Manual Dexterity | Fine motor skills | ||
| Balance | Gross motor balance | ||
| Aiming and Catching | Eye–hand coordination | ||
| Early literacy and numeracy: | |||
| TOPEL Print Knowledge | [48,49] | Letter names and sounds | Standard score |
| TOPEL Phonological Sensation | Ability to identify phonemes | Standard score | |
| DAS-Two Early Number Concepts | [44] | Counting and math trouble solving | T-score |
| Behavior ratings: | |||
| Conners EC-P Total Problems, Inattention/Hyperactivity, Anxiety, Social Performance | [36,42] | Symptoms of overall problems and in areas of attention, externalizing, and socialization | T-scores |
| BRIEF-P Global Executive Composite, Inhibitory Self-Control Index, Flexibility Index, Emergent Metacognition Alphabetize | [l] | Behavior symptoms of executive dysfunction | T-scores |
| ERC Lability/Negativity, Emotion Regulation | [39] | Symptoms of mood lability and ability to regulate emotions | Raw scores |
Table 3. Group differences in readiness measures.
Table 3. Group differences in readiness measures.
| VPT Grouping | FT Group | ||||
|---|---|---|---|---|---|
| School Readiness Measure out | M (SE) | M (SE) | β | p | Cohen's d |
| Global/cognitive ability (DAS-2): | |||||
| Full general Conceptual Ability | 92.17 (1.88) | 108.97 (ii.08) | −sixteen.80 | <0.001 | −1.29 |
| Verbal Power | 97.17 (one.97) | 107.12 (2.21) | −ix.95 | 0.002 | −0.72 |
| Nonverbal Power | 95.63 (2.02) | 108.29 (two.22) | −12.66 | <0.001 | −0.92 |
| Spatial Ability | ninety.08 (1.88) | 106.03 (2.05) | −fifteen.95 | <0.001 | −ane.23 |
| Executive function and processing speed: | |||||
| DCCS Age Corrected | 94.53 (2.15) | 100.05 (2.x) | −5.52 | 0.078 | −0.42 |
| DAS-Two Recall of Digits-Frontwards | 43.94 (1.77) | 56.75 (1.98) | −12.81 | <0.001 | −1.22 |
| Go No Become | 0.62 (0.03) | 0.75 (0.03) | −0.xiii | 0.003 | −0.70 |
| CTOPP−2 Rapid Symbolic Naming a | 96.15 (2.80) | 105.67 (2.77) | −16.68 | 0.031 | −0.57 |
| Motor skills (MABC−2): | |||||
| Total | five.52 (0.42) | eight.91 (0.45) | −3.39 | <0.001 | −1.18 |
| Manual Dexterity | 4.90 (0.42) | eight.29 (0.47) | −3.forty | <0.001 | −1.sixteen |
| Balance | six.92 (0.xl) | 9.61 (0.46) | −ii.69 | <0.001 | −0.96 |
| Aiming and Communicable b | eight.59 (0.43) | 10.46 (0.51) | ane.93 | 0.043 | −0.79 |
| Early literacy and numeracy: | |||||
| TOPEL Print Knowledge | 96.80 (2.22) | 107.26 (2.39) | −10.46 | 0.003 | −0.69 |
| TOPEL Phonological Awareness | 92.37 (ii.08) | 106.53 (ii.31) | −fourteen.sixteen | <0.001 | −i.00 |
| DAS-Ii Early on Number Concepts | 45.29 (one.27) | 55.89 (1.49) | −x.threescore | <0.001 | −i.31 |
| Behavior ratings: | |||||
| Conners EC-P Global Alphabetize Full | 56.23 (1.69) | 55.23 (one.88) | 1.00 | 0.702 | 0.09 |
| Conners EC-P Inattention/Hyperactivity | 55.81 (1.72) | 56.42 (1.97) | −0.61 | 0.822 | −0.05 |
| Conners EC-P Anxiety | 56.88 (1.74) | 55.46 (1.93) | 1.42 | 0.598 | 0.thirteen |
| Conners EC-P Social Functioning c | 53.73 (1.29) | 47.68 (1.48) | −12.61 | 0.001 | 0.64 |
| Brief-P GEC | 58.55 (1.66) | 51.31 (1.91) | 7.24 | 0.007 | 0.61 |
| Cursory-P Inhibitory Self-Command Alphabetize | 56.threescore (1.76) | 51.89 (ii.00) | iv.71 | 0.092 | 0.38 |
| BRIEF-P Flexibility Index | 54.67 (1.53) | 50.04 (i.73) | 4.63 | 0.056 | 0.43 |
| Cursory-P Emergent Metacognition Index | sixty.18 (ane.59) | 51.42 (one.91) | 8.77 | 0.001 | 0.76 |
| ERC Lability/Negativity | 27.74 (0.95) | 26.58 (1.10) | 1.15 | 0.447 | 0.17 |
| ERC Emotion Regulation d | 26.31 (0.40) | 28.39 (0.48) | iii.57 | 0.003 | −0.60 |
Table 4. Group differences in rates of deficits in school readiness.
Table 4. Group differences in rates of deficits in school readiness.
| VPT Group (n = 53) | FT Group (north = 38) | |||
|---|---|---|---|---|
| Area of Deficit | N (%) | N (%) | p | OR (95% CI) |
| Global/cognitive power (DAS-II): | ||||
| General Conceptual Ability | 16 (31) | 0 (0) | 0.017 | 31.85 (1.85, 548.forty) |
| Verbal Ability | 9 (18) | 0 (0) | 0.037 | 20.84 (1.21, 358.86) |
| Nonverbal Ability | ten (20) | ane (3) | 0.021 | x.96 (1.43, 83.82) |
| Spatial Ability | 20 (42) | 1 (iii) | 0.014 | xiv.x (one.73, 115.11) |
| Executive office and processing speed: | ||||
| DCCS Age Corrected | eleven (26) | 3 (8) | 0.040 | 5.00 (1.07, 23.29) |
| DAS-Two Recall of Digits, Forward | xiv (28) | i (3) | 0.007 | 15.43 (2.09, 113.90) |
| Become No Go | 16 (37) | ii (half-dozen) | 0.013 | 6.67 (one.49, 29.86) |
| CTOPP-two Rapid Symbolic Naming | 6 (18) | 3 (nine) | 0.654 | 1.39 (0.33, 5.91) |
| Motor skills (MABC-2): | ||||
| Total | 33 (62) | 6 (16) | <0.001 | 1.61 (1.31, 1.98) |
| Transmission Dexterity | 39 (74) | ix (24) | <0.001 | 1.58 (ane.27, 1.97) |
| Balance | xviii (34) | 6 (xvi) | 0.050 | one.22 (1.00, 1.48) |
| Aiming and Catching | 17 (32) | 2 (5) | 0.003 | one.25 (1.08, i.45) |
| Early literacy and numeracy: | ||||
| TOPEL Print Knowledge | fourteen (28) | one (3) | 0.043 | ten.08 (one.08, 94.43) |
| TOPEL Phonological Awareness | 13 (26) | 0 (0) | 0.031 | 22.87 (one.33, 394.68) |
| DAS-2 Early on Number Concepts | 12 (24) | 0 (0) | 0.039 | twenty.00 (1.17, 342.69) |
| Behavior bug: | ||||
| Conners EC-P Global Alphabetize Full | 16 (thirty) | 8 (21) | 0.888 | 0.92 (0.28, iii.04) |
| Conners EC-P Inattention/Hyperactivity | 20 (38) | 10 (26) | 0.666 | 1.25 (0.46, 3.38) |
| Conners EC-P Anxiety | 19 (36) | 9 (24) | 0.442 | ane.53 (0.52, iv.47) |
| Conners EC-P Social Functioning | 17 (32) | 1 (three) | 0.033 | 14.77 (ane.24, 176.29) |
| Brief-P GEC | 28 (53) | iv (eleven) | 0.001 | 6.90 (2.ten, 22.72) |
| BRIEF-P Inhibitory Self-Control Index | 25 (47) | half dozen (16) | 0.039 | iii.34 (1.07, 10.48) |
| Brief-P Flexibility Index | 18 (34) | iv (11) | 0.146 | 2.63 (0.71, 9.69) |
| Brief-P Emergent Metacognition Index | xxx (57) | 3 (8) | <0.001 | 12.81 (iii.lxx, 44.33) |
| ERC Lability/Negativity | 12 (23) | v (xiii) | 0.577 | 1.45 (0.39, five.42) |
| ERC Emotion Regulation | 13 (25) | 1 (3) | 0.002 | 1.22 (1.08, ane.39) |
| Multiple Deficits: | 44 (83) | 12 (32) | 0.001 | 1.42 (1.xv, 1.76) |
Table 5. Model fit statistics for latent grade analysis (LCA).
Table v. Model fit statistics for latent class analysis (LCA).
| Fit Statistics | Course 1 | Class 2 | Grade 3 | Class 4 | Form 5 |
|---|---|---|---|---|---|
| AIC | 8224.109 | 7972.723 | 7890.293 | 7843.928 | 7807.723 |
| BIC | 8298.268 | 8086.28 | 8043.248 | 8036.28 | 8039.472 |
| SSA-BIC | 8197.413 | 7931.845 | 7835.233 | 7774.686 | 7724.298 |
| Entropy | - | 0.944 | 0.963 | 0.966 | 0.958 |
| LMR | - | 285.385 | 116.43 | 80.365 | 65.277 |
| p-value (LMR) | - | 0.01 | 0.27 | 0.57 | 0.77 |
| BLRT | - | 285.385 | 116.43 | 80.365 | 65.277 |
| p-value (BLRT) | - | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
| Publisher's Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 past the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Source: https://www.mdpi.com/2227-9067/9/3/323/htm
0 Response to "Let the Random Variable X Represent the Number of Boys in a Family With Three Children"
Post a Comment